|
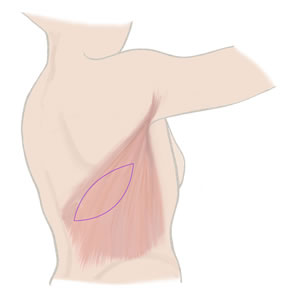
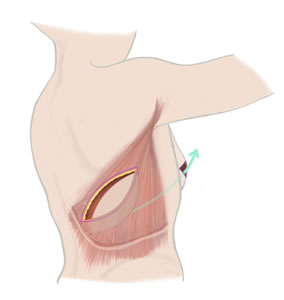
With this option, the tissue from the back (the latissimus dorsi muscle) is used to reconstruct the breast, either with or without an implant.
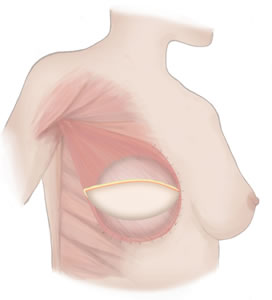
First, the tissue (located at the back of the shoulder blade) is brought around to the breast mound to create the new breast. Then, depending on the desired breast size, an implant is inserted underneath, as the latissimus dorsi does not always provide enough volume. It can also create a more natural breast shape. The scar is usually horizontal, so it can be hidden under bra straps. Occasionally, it is diagonal and therefore more difficult to cover.With this option, the tissue from the back (the latissimus dorsi muscle) is used to reconstruct the breast, either with or without an implant. |
|||
 |
 |
 |
 |
The advantages
|
And the disadvantages?
|
Latissimus Dorsi Muscle Reconstruction – overview |
|
| Operation time: | Normally between 3 and 5 hours |
| Hospital Stay: | Between 5 and 7 days |
| Type of Anaesthesia: | General anaesthetic |
| Recovery Time: | Around 6 to 8 weeks |
| Risks of Surgery include: | Bruising and swelling. Scarring.
Less common problems include infection and haematoma. Seroma (swelling in the back where blood/body fluid has collected) is more common. When lymph nodes are cleared, there’s sometimes a risk of lymphedema. Other risks include loss of the skin flap that’s been used for the reconstruction; blood transfusion (unlikely); shoulder and back stiffness; aches and pains; implant extrusion (when the body rejects the implant); and capsular contracture (excessive or invasive scar tissue formation). |
| Further Treatment: | Check up with your surgeon/registrar.
Visits to the Hospital Dressing Clinic. Regular visits to Outpatients department for injections if tissue expanders are used. In some cases, a second operation to replace the tissue expanders with a permanent implant |
| Nipple reconstruction: | Around 3 months later |
| Nipple Tattooing: | 1 month after reconstruction (by your surgical team) |